
Pragmatic Solutions for Tactical Performance Training
Pragmatic Solutions for Tactical Performance Training
Part 2: Post-Deployment Cycle

Part 2: Post-Deployment Pragmatism
Post-Deployment Phase
Let’s use an Airborne Infantry unit coming back from a 90 day deployment as an example. Upon return, my theoretical team would gradually begin testing everyone in the unit to gather data to guide recovery decisions and then training decisions. Generally, the qualities that we would want to work on first would be “Zone 2” aerobic capacity - more on heart rate zones later - and nervous system recovery, both autonomic and central. ANS/CNS recovery is actually enhanced by Zone 2 training, so the two work symbiotically.
Zone 2 - A Primer
Many endurance sport training models are designed around “heart rate zones,” where an athlete will do some baseline testing to find certain heart rate thresholds and the coach will assign training based on where the athlete’s different zones are. During an initial training cycle, the main emphasis is on developing what’s called an aerobic base and in endurance sports, this is classically referred to as “long slow distance,” with the goal being keeping the athlete’s heart rate in “zone 2” which is usually 60-75% of an athlete’s maximum heart rate. As “aerobic base” might imply, this training is foundational.
Nervous System Function
The hyper-vigilance that being in a combat zone requires is extremely stressful for the autonomic nervous system. The ANS functions on a continuum between sympathetic - fight, flight, freeze - and parasympathetic - rest and digest; with combat operations skewing heavily and continuously toward sympathetic arousal. In our scenario, chronic sympathetic arousal would result in disrupted sleep, immunosuppression, excessive “reactive oxygen species” which exist in a perpetual inflammatory environment within cells. The central nervous system provides nerve signals for bodily functions and movements. Sympathetic nervous system arousal can lead to high levels of CNS arousal as well, characterized by anxiety and poor performance on psychomotor vigilance tests, such as the tap test - performed via smartphone app. A simple CNS assessment would be a vertical jump, where a soldier jumps as high as he/she can and jump height is measured against previous jump heights. Decreases of more than 10% would be expected post-deployment and would warrant intervention.
Aerobic Threshold Testing - VT1
With running accounting for almost all of a soldier’s conditioning training but heart rate monitor access being sporadic at best, a practical solution is a ventilatory/aerobic threshold test. In a ventilatory threshold test, an athlete or soldier will begin running at a very low intensity where conversing in full sentences without breathing disruption is easy. After 10-15 minutes, increase intensity/pace slightly for 3 minutes while nasal breathing. After 3 more minutes, increase intensity/pace again while still nasal breathing. After 1-2 more 3 minute increments of increasing intensity, nasal breathing should become unmanageable. At this point, decrease intensity slightly to where nasal breathing is manageable, but still challenging. Maintain this intensity for 15 minutes and if the athlete/soldier has a heart rate monitor, make sure they note their average heart rate during this time period. If the athlete/soldier does not have an HRM, make sure they note their perceived exertion - or RPE - which will be identified as a 7 on a scale of 1-10. After 15 minutes of steady state, gradually decrease intensity for 5-10 minutes to cool down. The average heart rate or RPE from the 15 minute test period is identified as the top of Zone 2 and conditioning prescriptions will be based off of that data.
Sample Training
Using the data from the above assessment, a sample program for nervous system recovery is outlined below.
Non-Consecutive Training Days

Consecutive Training Days - Traditional 4 Day PT Schedule
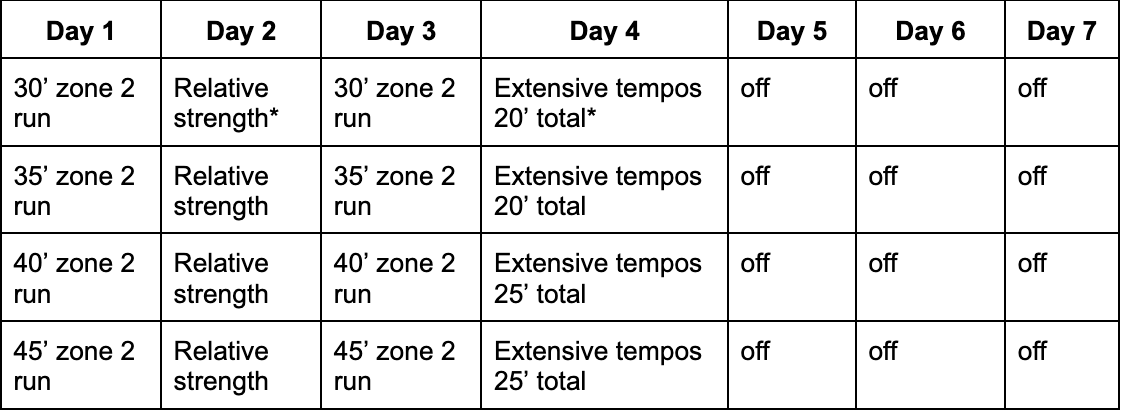
* Relative strength circuits include: pushups, pull-ups, air squats, lunges, lateral lunges
** Extensive tempos: 4-5x4:00 at 8RPE; 1:00 walking recovery
